Long-term psychological consequences due to problematic fetal period and birth
By Sanne Lundberg
Anton’s mother: “Is it normal not to be able to remember anything from your pregnancy and the birth?”
This article describes the treatment of a delicate and sensitive child who, as a fetus and infant, was exposed to violently traumatic events that had psychological consequences for him, which later threatened his cognitive development. I describe in the article what considerations I made and how I approached the treatment. I connect theory to practice based on the attachment theory and the neuroaffective development theory. I use various therapeutic methods, for example Theraplay, as well as elements from, among others, Somatic Experience (SE), where it is relevant. When I do this, I focus on how the two therapeutic approaches can complement each other during treatment. In the last part of the article, I discuss which elements during the treatment led to qualitative shifts in relation to the goal of the treatment in developing and improving the interaction between the parents and the child.
It was my meeting with three-year-old Anton, and his parents’ description of Anton’s regulatory difficulties and delayed development that aroused my professional curiosity in examining whether the mother’s difficult pregnancy and birth could be the cause of some of these challenges.
The parents had known each other for a short time before the mother became pregnant. They told me that Anton was a planned child. Anton’s mother said that the period after Anton’s birth was erratic and precarious, including moving to a new house. Anton started in day care at six months. The mother described Anton as almost apathetic during the period when he was in daycare. The daycare then changed to a nursery, due to the family moving when Anton was twelve months old. The teachers in the nursery slowly discovered that Anton was a sensitive and vulnerable child, and he was referred to Theraplay treatment with me via PPR. (Educational Psychological Counseling)
Both parents said they had been personally challenged throughout their upbringing and continued to be so in their adult lives. Anton’s mother explained to me that her teenage years had been difficult and her relationship with her own mother had been and continues to be difficult.
THERAPLAY
Theraplay is an interactive, relationship-based play therapy based on attachment theory. Its essence is the healthy, balanced interaction between parent and child. In Theraplay, the here-and-now experience of the interaction between the child and the primary adult is considered a goal in it self. The games and activities that the Theraplay sessions are built around, thus aim to initiate the neural network and thus the child’s opportunity to participate in healing and healthy moments of meeting. Source: theraply.dk.
It’s extremely remote from me – I can barely remember the pregnancy.” – “They could never find him, those scanning women.” “I think I could feel him five times in all during the whole pregnancy, and yet I doubted if it was him.
ANTON’S MOTHER ABOUT PREGNANCY AND BIRTH
Professionals point out that the time in the womb is probably the most significant period in a person’s life (Brodèn 2004, Levine and Kline 2012). An increased stress and alertness during pregnancy can mean that it takes less to stress the baby later on in life. In other words, we humans are shaped not only by our genetic predisposition, the environment and the people we meet after birth, but to a large extent also by the time in the womb – for better or worse.
Having the first child is often a challenging period in a woman’s life, and here calm, confidence and security are important for the woman to produce the hormone oxytocin. Oxytocin contributes both to the woman having good, effective contractions, and to the mother and child being connected to each other. If parents are stressed during the progress of a normal birth, the risk of complications during the birth increases.
If the woman has no notions of herself as a mother, or her own mother, the woman may lack a positive mother figure to identify with. Daniel Stern (2004) writes about the ‘constellation of motherhood’, which is an expression of the mind getting ready for a new kind of life with a child. The mother’s sensitivity and contact with her own developmental history has sharpened, and she begins to fantasize very quickly during pregnancy about representations of the child she is expecting. Anton’s mother did not feel life during her pregnancy, and this may be one of the reasons why it was harder for her to give birth to him. The placenta was in front, and Anton was lying and ‘hiding’ behind it. At the same time, the mother’s statements showed that she had been in doubt as to whether Anton was alive at all, and this was probably reinforced by the fact that the midwives often could not feel life either. One hypothesis may be that Anton’s mother was afraid to attach herself to Anton for fear of losing him again. Anton’s mother did not manage to fantasize about the expectant child therefore her mind did not manage to “reconstruct” during pregnancy.
In Ghosts from the Nursery: Tracing the Roots of Violence (2012), authors Robin Karr-Morse and Meredith S. Wiley presented compelling research that aims to awaken us and make us aware of the vulnerabilities of the first 33 months of life (fetal and the first 24 months).
Those mothers who had a weak or no prenatal attachment did not, by themselves, develop an attachment to the child after birth. A birth that was perceived as more difficult than expected affected the initial feelings for the child (Brodén 2004).
About the birth, the mother said: “It was just twelve hours of excruciating pain, I thought I was going to die, something was wrong, he was pressing in a strange way – I did not dare to let go and press, but in the end I pressed and pressed, and also without contractions, and ended up breaking completely inside – I was unprepared – could not recognize the pain – felt lonely and not heard – Anton was stuck in the birth canal – I did not care for him when he was born. ”
All women who give birth have a history, and we know that giving birth can reactivate past trauma (Levine and Kline 2012) Only the women who have given birth can determine whether their birth has been traumatic.
What triggers a traumatic reaction is when the person in question has felt helpless, terrified, offended, afraid of losing their life, powerless, and has lost self-control. Anton’s mother thought she was going to die. Her rationalization could not calm her or her surroundings, and she chose to ‘get out of her body’ – a dissociation that happens when everything is too overwhelming and there is no way out of the situation. She could neither escape nor fight. Anton’s mother was unprepared and for some reason had not formulated her wishes with her husband before the birth. Her unbearable pain overshadowed all joy. She felt she was losing all control and turned the aggression inward with a violent feeling of loneliness. Her husband did what he could to support her, but she described him as paralyzed and not heard by the system.
When the birth was finally over, she did connect with her child. She barely registered him in her exhaustion and helplessness.
MY MEETING WITH ANTON
When I met Anton as a three-year-old, my first impression was that he was a child with great difficulty. His body was tense, and he was on his toes. It did not take much stimulation before he was overstimulated. He could only make a little bit of eye contact. He let out chattering sounds and loud screams. Occasionally he came up with words, such as “no”, “yes” and “woof-woof”. He was uncritical in his contact with adults, and most of all, I perceived him as chaotic, unregulated, and on guard when it came to attuning to his surroundings.
The parents were seriously concerned about their son’s development and feared that he was brain damaged. Where they experienced him at his best was when he sat alone by himself and experimented with something. They told me that they had gradually accepted Anton’s repeated rejections and had given up participating.
Anton’s nervous system was on overtime during the birth. The amygdala, our alarm center in the brain, was constantly triggered, and a hypersensitivity had occurred, so that with every stimulus the signal was sent: “Danger ahead, danger ahead”, and the fight / flight system was switched on. Once the danger has passed, the body usually lowers its production of the combat hormones cortisol and adrenaline and returns to its normal state.
It seemed that Anton’s nervous system was not functioning normally. His overactive (sympathetic) autonomic nervous system was constantly highly activated and could hardly be regulated and calmed down. Anton’s restless nervous system ‘infected’ the parents and thus prevented the parents from creating safety and security for their child.
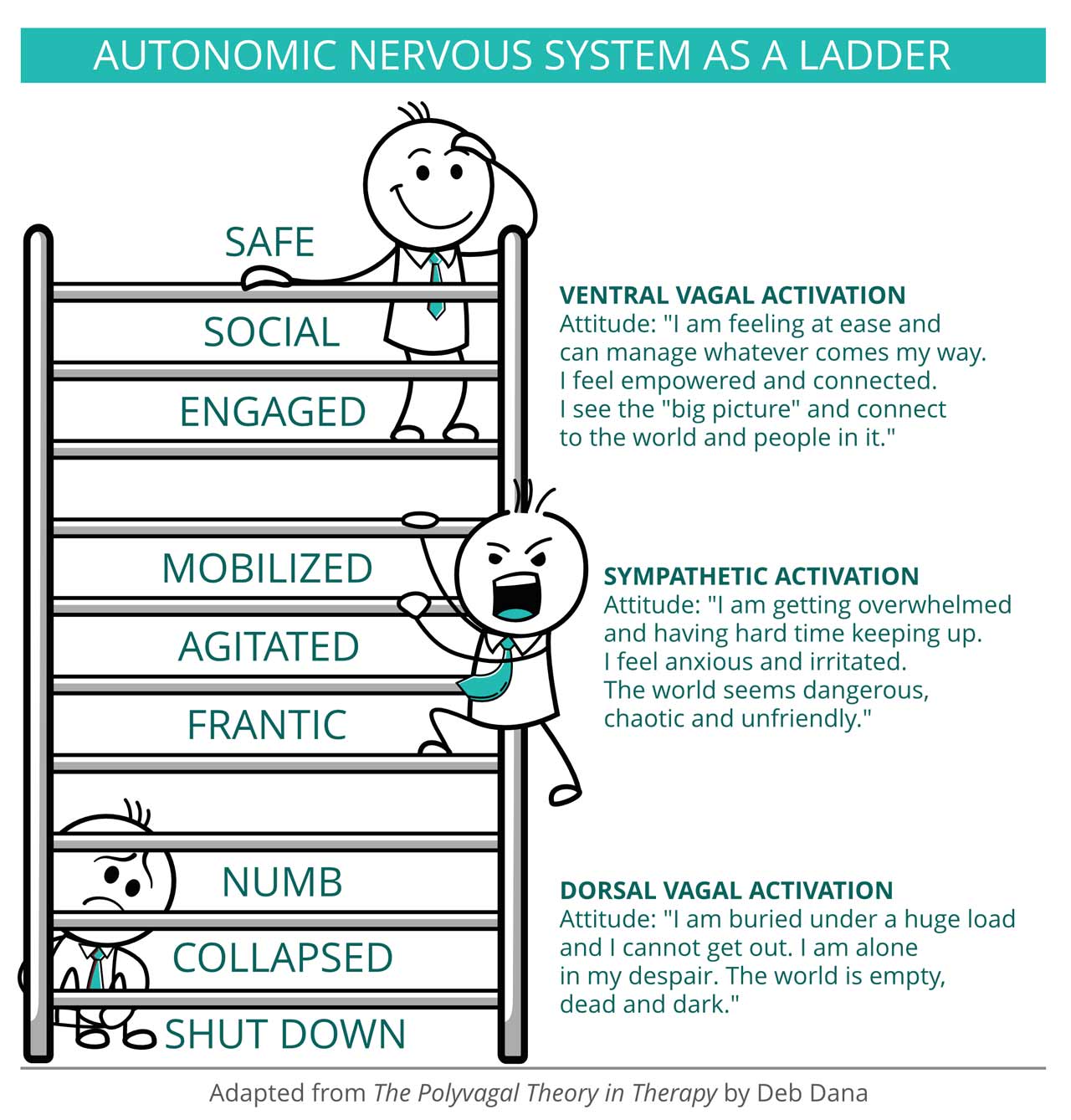
According to Porges’ theory, the part of the nervous system called the dorsal vagus is activated when we are threatened and feel in mortal danger but are unable to escape or fight. The dorsal vagus puts the body in a state of immobilization, i.e. it freezes or collapses, which can cause a dissociation by making one disappear into oneself / shut down from the outside world. The dorsal vagus response is the most primitive stress response we have and part of the parasympathetic response (Dana 2018).
For the first 3-5 years, the child needs its primary caregivers to activate the Social Engagement System. All newborns call their primary caregivers by crying or alerting discomfort. The caregiver satisfies the child’s needs, and the child is regulated. Thereby, a mutual attachment is felt, and both parties feel loved (co-regulation). Anton could not be regulated, and his social engagement system was not activated –
the interaction between Anton and his parents, who were supposed to calm him down, failed, probably due to his extreme sensitivity to stimulation.
The parents described that Anton disappeared ‘into himself’ from an early age, and they found that he sought this condition more and more. Anton’s passivity started already during the birth, where he was probably stuck in the birth canal, and here a shutdown took place. Already from birth, Anton had learned to shut down, and this dorsal-vagal-shut-down strategy instinctively followed him when he was overstimulated. Almost all stimulation became too much and thus “dangerous” for his nervous system.
COURSE OF TREATMENT
Something had gone wrong in Anton’s early start in life. I judged that Anton was emotionally, but also developmentally, far younger than three years. Both Anton and especially his mother had deep traumas from the pre- and postnatal period. Where should I start? Anton was three years old and had been in ‘no man’s land’ for a long time. His parents had done everything they could to help him, but Anton was so challenged developmentally that far more was needed than his parents could provide.
In relation to the Theraplay treatment, there was most success with small simple imitation activities. Here Anton showed short-lived curiosity and interest. Anton could not find physical calm anywhere, and so we wrapped him in a warm and soft blanket in a tow wagon. Small rides in nature relieved Anton, and opportunities were created for “moments of meeting” between Anton and his mother. Everything was at a very slow pace with small rhythmic activities. Slowly, Anton could approach his mother physically, for example sitting on her lap, but with his back to her at first. Direct contact for him was too overwhelming. If Anton had too much stimulus, he could continue to be overwhelmed, frustrated, unregulated or shut down completely.
After a few months, Anton could be gently introduced to small sensory activities, such as sitting on his mother’s lap and touching sand, modeling wax and the like. Live animals, such as dogs and horses, were involved in the treatment, and their presence had a further calming effect on Anton. Slowly, Anton could begin to feel himself and sought care and comfort when he became insecure and anxious (see illustration above). In the past, he just screamed or ran away and hid when he needed care.
Anton now dared to move around in his Circle of Security, and instead of fleeing he returned to the ‘safe harbor’ and into his mother’s open arms. His mother became more and more competent and dared to be the ‘caravan leader’ for Anton, even though she feared Anton’s protests and cries. The crying she had heard for almost his entire first year of life had affected her nervous system, but slowly the good experiences took over overshadowing the ‘scary’ ones. Anton became more insistent on contact. He drew less and less into himself and began to invite his parents into play. For quite some time he played almost daily that ‘the baby crocodile was rescued by his mother’. It was touching to see that Anton through the game showed us that we were on the right track. He was gaining confidence and believing that the adults around him wanted the best for him. Slowly, Mom found that she could read and understand Anton’s signals. In Theraplay sessions, Anton began to synchronize with his mother’s nervous system. He spoke more words and one of his first words was ‘mom’.

THE SIGNIFICANCE OF BIRTH
The mother’s change was beautiful to follow – her eyes shone with love for Anton when she talked about him and when she looked at him. “I found my boy.” I encouraged her to talk her pregnancy and birth through with a doctor or midwife, but she wanted to share it with me. Subsequently, she was relieved and surprised that she dared to talk about Anton’s early start in life and in that way process some of the traumatic experiences by working with herself physically via the SE elements (Somatic Experiencing).
Anton continued to reject his mom when he was stressed, and it was as if this rejection strategy of pushing and kicking was haunting him, especially when he got frustrated.
With inspiration from Peter Levine (2012) I considered whether it was the case that Anton had been cheated during his birth to perform his instinctive movements, so that the impulses and rhythms were never met, so that the natural rhythm during his birth had not been established.
The labor pains involve a synchronized effort of mother and child, with contractions, pressure, and rest. If the energy mobilized to begin the downward journey is never used, the child begins his life with impulses that have not been met (Levine & Kline 2012 p.278). Anton’s path must have been difficult for him. He was stuck in the birth canal for a long time as the mother was afraid to let go, and when she finally did, he came into the world forcefully and quickly. If shut down occurs as early as in the birth canal, it may become the baby’s preferred strategy when overstimulated. Anton was deprived of all redemption by not completing and ending the instinctive impulses and movements as one should.
With the help of the therapist and his mother, could Anton perhaps relive his own birth at a much calmer pace and this time allow himself to be caught in his mother’s arms? I made a setup where Anton had to pass through a fabric tube with a slight resistance of hands-on head, forehead and back. Anton’s mother fully agreed with that idea. Anton crawled purposefully and with strength and energy through the tube and ended up in his mother’s arms.
After this session, Anton’s mother experienced that Anton’s rejection impulses subsided. It was clear to me as a therapist that the session in combination with the Theraplay sessions had had a great impact on Anton’s progression.
CONCLUSION
Anton was in treatment for a year, and at the end of the treatment, the mother said the following:
“I know Anton loves me and it’s reciprocated.” – “Anton can concentrate and stay focused, and he enjoys being read to and singing songs.” – “Anton is creative in his games and has become incredibly good at role and fantasy play.” – “Anton’s language has developed incredibly, with many words and sentences.” “Anton understands everything I say to him, and he often surprises me with his sense of humor.”
In the article, I have sought to describe how I use my theoretical approach in different ways to solve the different problems that the child and parents are challenged by. I hope the article has provided an insight into what can happen if the child and parents are not ‘detected’ before an erroneous development occurs.
We should pay attention to:
• The importance of starting a healing when there has been a difficult start in life.
• The importance of repairing the difficulties the child has had in the early start of life.
• The importance of not giving the baby a diagnosis before considering and examining whether there have been any disruptions during pregnancy and birth.
• That we professionals both ‘see and hear’ parents who experience the birth as difficult and traumatic, even though we see it as relatively unproblematic.
• That we as professionals spot parents and children’s interaction difficulties before a maldevelopment occurs.
Anton and his parents are probably not finished with their treatment, and they will need further support. Every child has the right to a secure and safe attachment with their primary caregivers, and this has been achieved for Anton – he has become attached to his parents and vice versa.
I have chosen the following quote from Levine and Kline’s Trauma seen through the eyes of the child because it very nicely sums up exactly what I witnessed as a therapist for Anton and his mother: “Children are born with inner resources, but are dependent on, that the adults (an external resource) mirror them and take care of them so that they become visible.” (2012).
Thanks to Anton’s parents for permission to share their difficult story with other professionals, so that we as therapists can become more aware of how a problematic start in life can affect the individual human being. And thanks to my supervisor Ursula Fürstenwald.
LITERATURE
Brodén, Margareta: The possibilities of pregnancy. Akademisk Forlag 2004.
Hart, Susan: The Importance of Cohesion. Hans Reitzels Forlag 2006.
Kolk, Bessel A van der: The body keeps accounts. Klim 2019.
Levine, Peter & Maggie Kline: Trauma seen through the eyes of a child. Dansk Psykologisk Forlag 2012.
Deb Dana: The Polyvagal Theory in Therapy W.W. Norton & Company 2018
Stern, Daniel: The Motherhood Constellation. Hans Reitzels Forlag 2004.